

Menstrual Cycles and Serotonin: Implications for Psychedelic Research
Study Suggests Increase in Serotonin Transporter Binding in PMDD Patients


A 2023 study published in Biological Psychiatry explored the relationship between the serotonin system and menstrual cycle phases in patients with premenstrual dysphoric disorder, or PMDD. Results show changes in the serotonin system based on menstrual cycle phase, posing interesting questions for psychedelic researchers working to better understand the serotonin system and it’s role in mental health.
PMDD affects an estimated 3-9% of reproductive aged women. Symptoms may include severe depression, suicidal ideation, severe anxiety, sensory sensitivity, and emotional lability as well as physical symptoms like headaches, swelling and painful periods. Symptoms present in the luteal phase of the menstrual cycle and are relieved within a few days of starting the period.
The study included 30 PMDD patients and 29 controls. Utilizing PET scan technology, researchers measured serotonin transporter density across menstrual cycle phases. Also referred to as SERT, serotonin transporter density refers to the amount of the protein that regulates serotonin levels through the reuptake process.
Serotonin reuptake is the primary target for serotonin reuptake inhibitors, or SSRIs. By inhibiting reuptake, SSRIs are believed to increase serotonin availability.
Results showed an increase in SERT density in key areas of the brain related to emotional processing in the PMDD group during the luteal phase of the menstrual cycle. The increase in SERT density correlated with depressive symptom severity, leading researchers to call for more research on pre-symptom-onset dosing with SSRIs.
Dosing
With PMDD, there is some evidence to support pre-symptom onset dosing with SSRIs. PMDD is unique in mental health because symptoms subside after starting a period, and SSRIs are sometimes prescribed during the luteal phase of the cycle rather than the entire month.
“Researchers observed that for the treatment of PMDD, SRIs seemed to work more rapidly, taking effect within a few days of treatment initiation (as opposed to the 2-4 weeks needed for the treatment of major depression).”
It is interesting that women with PMDD seem to respond differently to SSRIs. One possible explanation is the difference in serotonin uptake in women with PMDD - the drug might not need as much time to do the job. This anecdote should be considered as psychedelic research evolves; if PMDD peeps respond differently to SSRIs, compared to the general population, might they also respond to serotonergic psychedelics differently?
While it is still anecdotal, there are some reports of seasoned psychedelic users with PMDD lowering the dose during the luteal phase, if they do choose to consume during this time. This is a wise move for harm reduction, as the luteal phase is already a period of heightened awareness and sensory sensitivity for women with PMDD, and there is evidence for differences in the serotonin uptake.
On the other hand, some women with PMDD avoid perceptual psychedelics completely during the luteal phase, and opt for microdosing instead to help manage mood. This point is outlined further in a paper by Alana Cookman who interviewed women with PMDD who have experimented with perceptual dose psilocybin.
The Serotonin System is Trippy
Serotonin has long been indicated in mental health disorders, and approximately 1 in 6 Americans have used an SSRI. Serotonin is often referred to as the “feel good” neurotransmitter related to mood and well-being, but it’s role in the human experience is a bit more complex.
Heavily influenced by psychedelic research during the 50’s, the hypothesis suggesting that serotonin is involved in mental health disorders originated from a paper published in 1954:
“Mental disturbances caused by lysergic acid diethylamide (LSD) were to be attributed to an interference with the action of serotonin in the brain.” -Woolley and Shaw (1954)
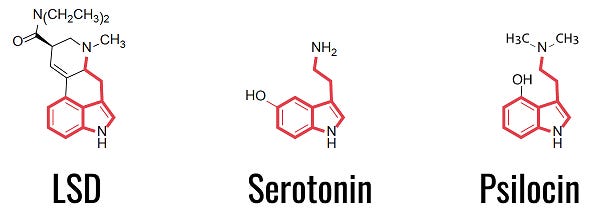
The discovery of LSD in 1943 and subsequent research on mental health led researchers to compare LSD’s experiential effects - including changes in sensory perceptions and hallucinations - with schizophrenic episodes. The molecular structure of LSD, serotonin and psilocin - a psilocybin mushroom metabolite - are similar.
While serotonin is well known for it’s role as a neurotransmitter - responsible for transmitting chemical messages across various biological processes including mood, sleep, learning, cognition and sleep - serotonin also acts a hormone.
In this context, one can reasonably argue that any condition believed to be caused by serotonin levels, or dysfunctional serotonin reuptake could also be considered hormonal, making PMDD one of many, hormone related conditions.
Serotonergic psychedelics like LSD and psilocybin mushrooms activate serotonin receptors and produce temporary altered states of consciousness, also known as “trips”. According to the idea that serotonin is involved in mood and well-being it makes sense that serotonergic activators (agonists) like LSD and psilocybin can increase euphoria and a feeling of well-being, but what about the other effects?
Why would a serotonergic psychedelic drug induce altered states of consciousness capable of surfacing past traumas, causing auditory and visual hallucinations, and leading to potential, nightmarish experiences? Perhaps psychedelics are working with more than the serotonin system, or perhaps, what we know about the serotonin system is incomplete.
Psychedelic scientists are working to better understand the role of serotonin in inducing various altered states of consciousness - and more importantly, how those experiences lead to clinical outcomes for mental health conditions. Psychedelic research helps scientists better understand how the serotonin system may impact mental health by activating it under different conditions with the use of serotonergic psychedelics.
“The best way to understand how a system works is to disrupt it and see what happens.”
- Michael Pollan
Psychedelic Research for PMDD
Psilocybin mushrooms were designated as a breakthrough therapy for treatment resistant depression in 2014 and are now legal for medical use in Oregon, Colorado Canada and Australia. Active legislation calling for decriminalization and /or legalization is ongoing in more than a dozen other US states.
While there is no formal research on PMDD and psychedelics, anecdotal reports and case studies from the PMDD community demonstrate that some women with PMDD use psychedelics to self-treat. In Canada, women with PMDD can access psilocybin therapy through a special access program available for severe mental health issues.
Psychedelics are a complex topic. For more information - including risks and harm reduction - check out our harm reduction guides:
Psychedelic assisted therapy is already a legal option for some women based on location, and for others - like myself - we can’t exactly wait for formal research to catch up, especially when standard treatments fail.
Psychedelic research on PMDD, and the menstrual cycle in general, is key to inform the development of new treatment options for menstrual related conditions, increase safety and efficacy while administering psychedelic medicines to women at healing centers, and to improve harm reduction information available for those of us already using psychedelics for PMDD.
For more information on this topic, check out my video, A Call for Compassionate Use: Psychedelic Assisted Therapy for PMDD. To stay up to date on research and advocacy efforts related to psychedelics and the menstrual cycle:
How interesting the similarities of the chemical compounds of LSD, pscilocin, and SSRI’s. I know many pharmaceuticals are influenced by the plant world. Thank you for this well-written post.